PTZ’s convulsive history

The pro-convulsant drug pentylenetetrazol or PTZ has a fascinating history. PTZ’s first medical uses in the 1920s predate the discovery of amphetamines. In the 1930s, it was used in psychiatric hospitals to deliberately induce seizures in people with schizophrenia. Decades later, it was advertised as a mild stimulant for the elderly, before being removed from the market as part of FDA reforms.
I did some research on PTZ for my upcoming book on idiopathic hypersomnia, because it was being tested in clinical trials for IH. Unfortunately Balance Therapeutics, the company that was developing the drug for Down syndrome and then IH, was dissolved, and it looks PTZ has come to a dead end. Starting in 2015, Balance conducted two studies of PTZ for sleep disorders, and if either had positive results, we would have heard about them by now.
That’s why I decided to cut some details about PTZ’s back story out of my book, as part of an effort to reduce word count. But I still think this material is intriguing, so I am posting it here, with a little embellishment.
Chemists in Germany and Finland first synthesized PTZ in an effort to find a more reliable and convenient alternative to camphor, then touted as a cardiac stimulant. Known first as Cardiazol and called Metrazol in the United States, it was manufactured by the German pharmaceutical firm Knoll. (In the 1970s, Knoll was taken over by BASF and then sold to Abbott in 2002.)
PTZ’s discoverers observed that high doses triggered seizures in animals. Smaller doses could counteract anesthetics or sedatives, such as chloroform or barbiturates. PTZ immediately found use in surgery. In 1925, a Düsseldorf surgeon reported giving the drug to various patients who had a weak pulse and were in danger of circulatory collapse. It was similar to how emergency medicine departments employ other drugs such as epinephrine or vasopressors today.

The person who brought PTZ to greater prominence was Ladislaus von Meduna, who was working at a psychiatric hospital in Budapest. Meduna had proposed that epilepsy and schizophrenia were neurobiological opposites. From pathology studies, he proposed that glial cells were hyperactive in epilepsy but less active in schizophrenia. He also surmised that the two conditions were mutually exclusive based on hospital populations. This idea led him to use PTZ to induce seizures in people with schizophrenia. Beginning in January 1934, he injected them with camphor, and later with PTZ, which was faster and more reliable.
Meduna claimed astounding results. In his autobiography, he described one of the first patients he treated, who had been in a catatonic stupor for four years. After induced seizures, the man was able to get dressed and converse, although he periodically relapsed into catatonia for the next several days. In his first publication, he reported that of 26 schizophrenic patients treated in this way, 10 recovered and in three, there was “great improvement.”
Psychiatrists in other European countries and the United States enthusiastically adopted his approach. By 1937, more than 1,000 patients had been treated with “convulsion therapy.” The procedure appeared to work especially well for catatonic patients, but was also tried for others diagnosed with schizophrenia and severe depression. At the time, psychiatrists had little to offer such patients. It was before the first antipsychotic drugs appeared in the 1950s.
Between PTZ injection and seizure onset, many patients experienced intense dread. Although they lost consciousness during the seizures themselves, some described the run-up as feeling like electrocution. The convulsions induced by PTZ were vigorous enough that as the practice spread, concern grew over broken bones. Disturbing videos of the practice are available online, including one from University of Nebraska School of Medicine in the 1940s.
Although the efficacy of PTZ-induced seizures against schizophrenia now appears doubtful, they were a precursor to electroconvulsive therapy (ECT), which is still practiced today as a treatment for depression. ECT has evolved significantly since that time.
The tired organism
Around the time convulsion therapy swept across psychiatric hospitals, doctors were finding other opportunities for lower doses of PTZ in sports. “The chief reason why athletes have resorted to this substance lies in its stimulating influence on the circulation and the central nervous system, which produces a definite subjective feeling of freshness in the tired organism,” a Danish physiologist wrote in a 1939 report on doping for the League of Nations.
A team physician reported giving the drug to Austrian Olympic soccer players, with “outstanding” results. On a German expedition to the Himalayas in 1931, one of the mountain climbers collapsed and could proceed only after taking the drug every two hours.
According to Norman Ohler’s 2017 book Blitzed: Drugs in the Third Reich, Nazi leader Hermann Göring took Cardiazol for dizziness. Göring, a morphine user, may have become familiar with PTZ through its use in emergency resuscitations. For Göring’s use of Cardiazol, Ohler relies on the diaries of physician Theodor Morell, seen as unreliable by some historians. Ohler writes that Hitler asked about Cardiazol but Morell refused him, thinking it was too risky.
PTZ was tested in Europe and the United States as a circulatory stimulant for patients undergoing general anesthesia, or as an antidote for barbiturate poisoning. Knoll distributed the drug in ampules for injection, with instructions for these uses: differential diagnosis of comatose states, rousing someone from narcosis, and seizure induction in psychiatry. PTZ was also combined with caffeine, ephedrine or quinine.
Gentle cerebral stimulation
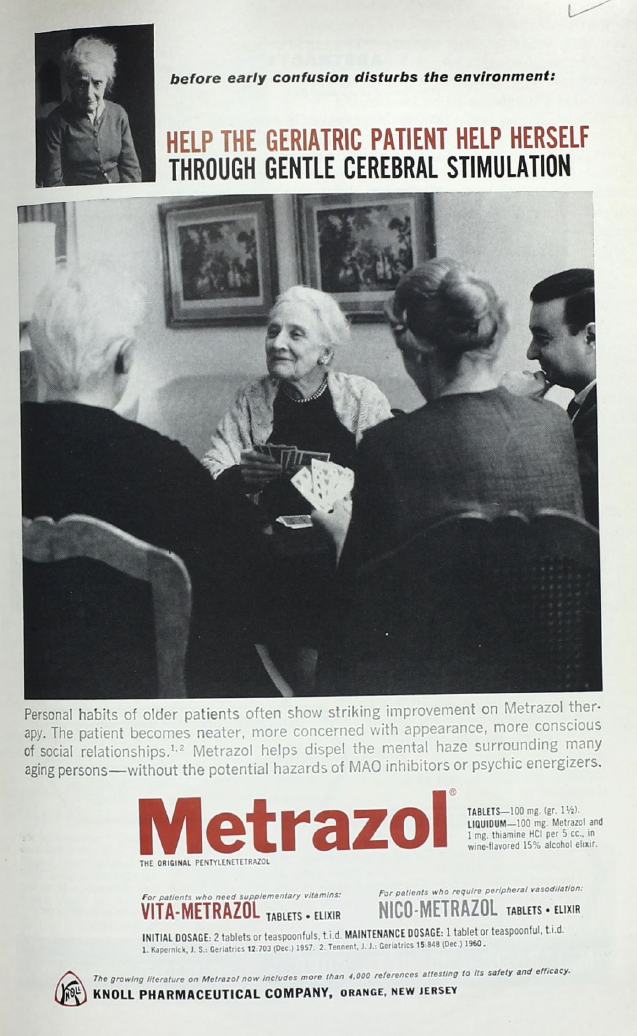
After seizure induction and sports doping, the next step in PTZ’s evolution may be surprising. In the 1960s, PTZ was promoted to doctors as an option for providing “gentle cerebral stimulation” to elderly people with dementia. The 1963 advertisement below was in the journal Geriatrics, with competing ads for Ritalin on other pages.
For PTZ, how did this transition happen? The first doctors in the United States to report on sub-convulsive doses for the elderly were at Cook County hospitals in the Chicago area. They cited its use in sports and wrote that they were concerned about caring for aged patients “who often are not only bedridden but mentally confused.”
In several subsequent studies, a gradual shift occurred toward people who were less impaired. Researchers rationalized the mechanism of action as coming from circulatory stimulation, “larval seizures,” or, given increasing understanding of neuroscience, from acetylcholine. Based on what we know now, acetylcholine was the wrong neurotransmitter, but they may have been headed in the right direction. Most of these studies would not be considered rigorous today, but were standard practice then.
An example from 1954, published in the New England Journal of Medicine by a Harvard Medical School instructor, included just 20 people, had no placebo arm, no blinding, and relied on the physician’s impressions of whether a patient was cheerful and cooperative. A physician at a Massachusetts state hospital reported: “We now give Metrazol to most of our geriatric patients as soon as they enter the hospital.”
Given PTZ’s past, doctors’ experience giving it to elderly individuals does provide some reassurance about the drug’s safety. One study included more than 600 patients, who took the drug every day for years with no seizures and few other adverse effects reported. The doses were lower, a fraction of a gram over the course of a day, compared to more than 10 grams for seizure induction typically — and the drug was administered by mouth, rather than by injection.
In several copycat formulations, PTZ was combined with the vitamin niacin and labeled as a treatment for vertigo. Still, Metrazol and its relatives were minor players commercially, compared to Ritalin and other stimulants, according to a 1968 U.S. government survey. A consensus formed that despite glowing reports on patients’ well-being, PTZ’s effects on cognitive measures were weak. In the 1970s, the FDA revoked approval for medications containing PTZ, citing the lack of rigorous clinical studies. A notice in the Federal Register reads:
“Virtually all of the products are offered for one or more conditions which may be associated with aging or senility; several are also offered for vertigo. Viewed collectively, the labeling offers the products as a panacea for conditions, both mental and physical, which may accompany old age.”
The drug appeared in a 1973 Supreme Court case (Weinberger vs Bentex Pharmaceuticals), part of a series of cases that ratified the FDA’s ability to decide the status of entire classes of products, bypassing federal courts. After that point, pentylenetetrazol was mainly used in animal research to study epilepsy.
Out of the dustbin
In the 21st century, scientists at Stanford revived PTZ as part of a burst of drug discovery efforts aimed at Down syndrome, which researchers had assumed for years was too complex and permanent for pharmaceutical treatment. PTZ displayed positive effects on memory in studies of a mouse model of Down syndrome, and was evaluated in a clinical trial in Australia (never published).
The rationale for PTZ as a treatment for idiopathic hypersomnia was that it should push back against overactive GABA signals in brain circuits regulating sleep and wake. Mechanistically, PTZ resembles flumazenil and clarithromycin, which get a lot of attention in my book. It is also related to 3-HMC, a GABA-A receptor antagonist investigated at the NIH in the 1980s, as well as flumazenil’s cousin sarmazenil, which Roche investigated as a potential wake-promoting medication in the 1990s.
PTZ differs from flumazenil in a critical way. It doesn’t act on GABA-A receptors’ benzodiazepine binding site — it directly blocks GABA-A receptor function and its action should not depend on the presence of a somnogenic ligand. PTZ’s pharmacology was different enough from conventional stimulants for it to be a possible alternative to them, but its success would not have proven David Rye’s “sleepy stuff” theory about hypersomnia.
